INTRODUCTION
Standard precautions are the gold standard guidelines designed to maintain a safe environment for patients, relatives, and healthcare workers. They are applied to all patients, regardless of their diagnosis or presumed infection status [1]. Infections acquired in healthcare settings are referred to as healthcare-associated infections (HAIs). They are acquired by patients for the first time either within 48 hours of hospital admission or 30 days after hospital discharge [2, 3]. They also include infections acquired within the hospital healthcare personnel [4].
Globally, 136 million healthcare-associated infections occur annually [5], with 9 million in Europe’s acute and long-term healthcare settings. Middle-income countries bore the highest annual burden, with 119 to 215 million cases [5], with 15 out of 100 patients acquiring healthcare-associated infections during hospitalization and 1 out of 10 dying [6]. The prevalence of HAIs in Africa is 12.76% [7] twice as higher than that of the developed countries while studies revealed that Nigeria has a 14.3% prevalence of healthcare-associated infection [8]. This prevalence is four times higher than that of developed nations and nearly twice the rate of healthcare-associated infections (HAIs) in Africa. Infection rates of 43.9% in surgical wards and 20.5% in medical wards were also reported in Nigeria [9, 8].
Healthcare-associated infections can be caused by bacteria, fungi, and viruses hosted by an immunocompromised patient and persons or indirectly contracted from hospital surfaces such as door knobs, tables, and other care equipment which come in contact with infected hands, other body parts, or pathogen’s route of exit from its reservoir [10]. These routes of exit are mucous membranes, non-intact skin, genito-urinary, gastrointestinal, and respiratory tracts [1] and can be transmitted to its victim in the hospital environment mainly through direct and indirect contact. Direct transmission primarily occurs through skin-to-skin contact, as well as airborne droplets
generated by coughing, sneezing, or talking [11], allowing pathogens to spread before settling on a surface such as oxygen cylinders, bedside tables, doorknobs, commodes, bed linens, bed rails, toilet apparatus, and mops and the ground [12]. Hospital waste such as blood, and body fluid stained refuse, blood bags, infected gauze, swabs, bandages. Additionally, sharp objects like needles, syringes, and blades also play a significant role in infection transmission [1]. Other sources of work-related injuries include cleaning chemicals, disinfectants, expired medications, and contaminated vaccines [13, 12, 14, 15].
Ancillary healthcare workers are responsible for hospital housekeeping responsibilities, transportation of patients, assisting health workers, and maintaining hospital cleanliness. They are also responsible for collecting, transporting, disposing of, and storing hospital infectious and hazardous wastes [16, 17]. These responsibilities expose them to cleaning and disinfecting chemicals, including quaternary ammonium compounds, bleach, and alcohol, blood and body fluids stained waste, needle and sharps [14, 18, 19].
Knowledge and practices of standard precautions for ancillary healthcare workers, such as Environmental cleaning and disinfection, have been confirmed to reduce the risk of pathogen transmission by lowering or eliminating hospital surfaces and equipment’s bio burdens [20]. Hand hygiene is another standard precaution involving washing hands with soap and water or using an alcohol-based hand rub to reduce bio burdens carried by the hands of healthcare workers, patients, and relatives, preventing the cross-transmission of infections between them [12]. PPE includes gloves, gowns, masks, and eye protection, they act as barriers preventing direct contact with infectious agents thereby reducing the risk of contamination. Proper Waste disposal ensures that medical waste is disposed of safely and properly according to local regulations and guidelines and reduces the risk of exposure to infectious agents for healthcare workers, patients, and the community [21]. Linen handling involves using precautions when handling, transporting, and processing soiled linen to avoid direct contact with skin and clothes, thereby minimizing the risk of pathogen transmission through contaminated textiles [12].
However, unpublished sources have confirmed poor standard precautions training for both newly employed and long-serving ancillary healthcare workers, cases of hepatitis B infections, and improper use of personal protective equipment (PPE) in a teaching hospital in Osun state. Studies also revealed that the ancillary healthcare workers exhibit the poorest knowledge and practices of standard precautions among healthcare workers. Among such identified were poor hand hygiene knowledge and practices, ineffective surface cleaning practices, poor personal protective equipment (PPE) usage [19, 22, 23,24, 25, 18, 26].
However, a study revealed that an intervention study on standard precautions specific to the roles and responsibilities of ancillary healthcare workers led to improved knowledge and practices of standard precautions among them [27]. Nevertheless, the majority of intervention studies conducted on knowledge and practices of standard precautions were carried out among professional healthcare workers such as doctors, and nurses students [28, 29, 30, 31,32]. The few intervention studies that included ancillary healthcare workers alongside professional healthcare workers emphasized standard precautions that were relevant to professional healthcare workers, while the key aspects specific to ancillary roles, such as environmental cleaning and disinfection, safe waste and linen handling, were largely neglected.
Poor knowledge and practices of standard precaution among ancillary healthcare workers have been reported to be associated with higher hospital surface bio burden, increasing asthma prevalence, skin disorders and a higher risk of transmission of hospital- acquired infections specifically the highly infectious hepatitis B [25, 33,34, 35, 36].
This study aims to determine the effect of a nurse-led intervention study on knowledge and practices of standard precautions among ancillary healthcare workers of a teaching hospital in Osun State.
Methodology
Study Area and population
The study population were the ancillary healthcare workers of Uniosun Teaching Hospital, Osun State, Nigeria. Their total population according to the Uniosun Teaching Hospital Records for the population of AHCWs, 2024, was 170.
Research Design
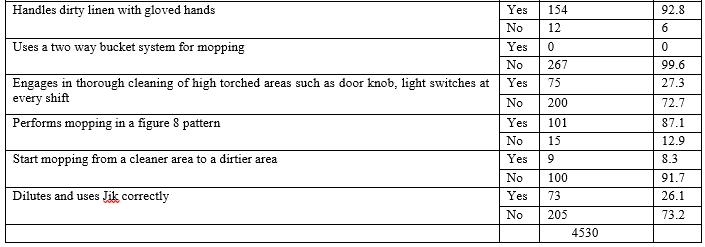
A quasi-experimental design of one-group pretest-posttest was used for the study Sample size determination Data on knowledge and self-reported practices of standard precautions were collected from 121 eligible participants across selected wards and units who willingly attended the training session and completed all aspects of the questionnaire. The sample size for direct observation of standard precaution practices was based on the WHO Hand Hygiene Technical Reference Manual [37], which recommends 200 observation opportunities per ward per observation period. Following this guideline, a minimum of 4,000 opportunities was necessary for the 20 selected wards. In total, 4,530 standard precaution opportunities were observed and documented.
Methodology
Study Area and population
The study population were the ancillary healthcare workers of Uniosun Teaching Hospital, Osun State, Nigeria. Their total population according to the Uniosun Teaching Hospital Records for the population of AHCWs, 2024, was 170.
Research Design
A quasi-experimental design of one-group pretest-posttest was used for the study.
Sample size determination
Data on knowledge and self-reported practices of standard precautions were collected from 121 eligible participants across selected wards and units who willingly attended the training session and completed all aspects of the questionnaire. The sample size for direct observation of standard precaution practices was based on the WHO Hand Hygiene Technical Reference Manual [37], which recommends 200 observation opportunities per ward per observation period. Following this guideline, a minimum of 4,000 opportunities was necessary for the 20 selected wards. In total, 4,530 standard precaution opportunities were observed and documented.
Subject inclusion and exclusion criteria
All ancillary healthcare workers deployed to the wards and units having standard precaution commodities sufficient for workers on duty, ran all three shift duties, and had worked for more than 6 months. Those on leave at the time of data collection and intervention.
The instrument for data collection
A structured, validated questionnaire and a checklist with a reliability Cronbach’s alpha coefficient ranging from 0.73 to 0.81 developed based on CDC (2024)’s Best Practices for Environmental Cleaning in Global Healthcare Facilities with Limited Resources, the CDC (2024) core IPC guidelines for safe healthcare delivery across all settings, and the OSHA (2023) guidelines on PPE usage were used to collect data, Pre- intervention (P1) and Post-intervention (P2). The questionnaire consists of three sections, including the socio-demographic data of the respondents, knowledge of standard precautions, and practices of standard precautions. The socio-demographic section had 10 questions on age, sex, marital status, religion, occupation, educational qualifications, work unit, length of employment, training on standard precautions, and the last time respondents had training. The knowledge scale was made up of multiple-choice questions with a total of 22 items. The scale measured knowledge of PPE usage for the roles of the ancillary healthcare workers, hand hygiene, surface cleaning and disinfection, medical waste management, sharp safety, hepatitis B prevention, and linen handling. A score of 1-11 was considered poor, and 12-22 was considered good knowledge of standard precautions. The practice section was a yes or no response scale with a total score of 28.
1-14 was considered poor and 15-28 was considered a good practice. It had items on self-reported actual PPE worn for housekeeping roles, hand hygiene performance, actual cleaning and disinfection practices, and linen handling. The checklist was a yes or no scale with a maximum obtainable score of 19.
Method of data collection
Ethical approval with protocol number: UTH/REC/2024/06/963 was obtained from the research settings to collect data. Pre- intervention, this approval was presented to the Directors of Nursing Services (DNS) to facilitate the release of ancillary healthcare workers under their supervision. Meetings were held with the heads of the ancillary healthcare workers to explain the study objectives, training components, and data collection procedures. These details were subsequently communicated to their respective staff members. An assessment of standard precaution commodities available per wards and units was conducted, and 20 wards that met the inclusion criteria were selected. Out of the 29 wards and units at the UNIOSUN Teaching Hospital, 20 were purposively selected for observational data collection based on the defined inclusion and exclusion criteria.
Training of the observer
Before commencing the observations, one observer per ward or unit (a total of 20) was trained on the AHCWs standard precaution guidelines. The training covered the CDC (2024)’s environmental cleaning procedure [38], the CDC (2024) core IPC guidelines for safe healthcare delivery across all settings [39], and the OSHA (2023) guidelines on PPE usage [40]. Observers were also assessed on their ability to conduct standard precautions compliance assessments using the structured checklist. The training included role-playing scenarios carried out by the researcher and two other infection control nurses based on the guidelines, focusing on key practices such as hand hygiene moments, selecting appropriate PPE for surface cleaning and disinfection, waste disposal, patient transportation, and proper preparation and use of cleaning solutions. Appropriate procedures for cleaning, mopping, surface disinfection, safe handling of bed linens, sharps, and medical waste were also role-played by the researcher and other experts and replayed by the research observers. Areas requiring amendments were collaboratively reviewed, discussed, and resolved. Pre-intervention data of observed practices of standard precautions were collected for two weeks using the structured checklist, while data on knowledge and self-reported practices of standard precautions were gathered immediate pre- intervention on the training day.
The educational intervention was delivered through lectures (presented by the researcher), audiovisual aids and hands-on practical sessions over two days, followed by an immediate post-training knowledge assessment. Standard precaution commodities were distributed based on ward needs. Posters on disinfectant dilution, ward mopping procedures, hand washing, and medical waste segregation were placed at strategic locations in the wards and units. Data on self-reported and observed practices of standard precautions were recollected at the 6th to 8th weeks post-intervention.
Data management
Data was analyzed using SPSS version 22. Descriptive statistics of frequencies and percentages were used to analyze participant’s socio-demographic data. Mean, standard deviations, and mean differences were used to analyze the research questions. Inferential statistics of paired t-test was used to analyze hypotheses at a 5% level of significance.
Results
Participant’s socio-demographic characteristics
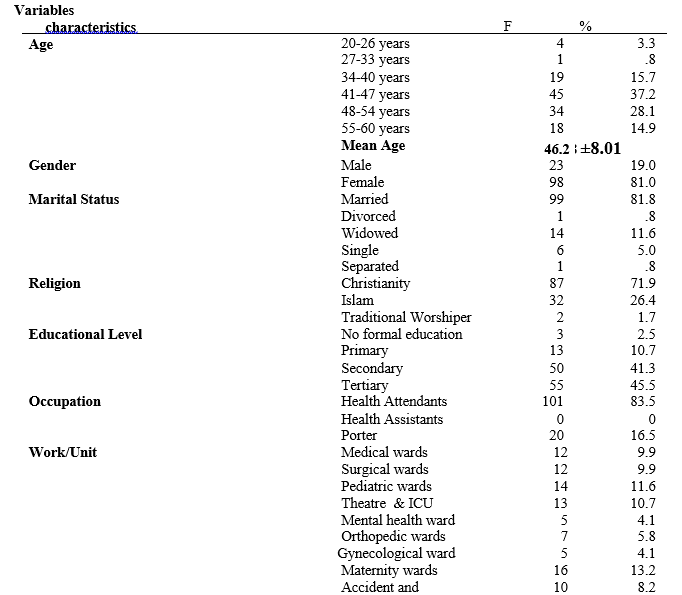
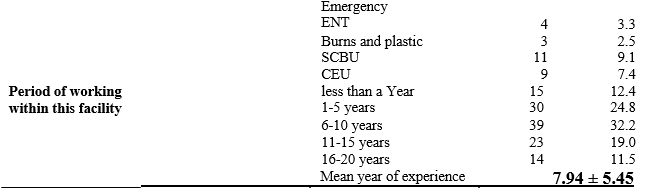
Of the 121 that participated in this study, 45 (37.2%) were between ages 41-47 years and 34 (28.1%) were between 48-54 years with a mean age of 46.28 ±8.01). The majority 101 (83.5%) reported having received SP training, however, a higher proportion, 52 (43.0%) reported that their last training was over three years ago, 20 (16.5%) had never received any training, Table 1a.
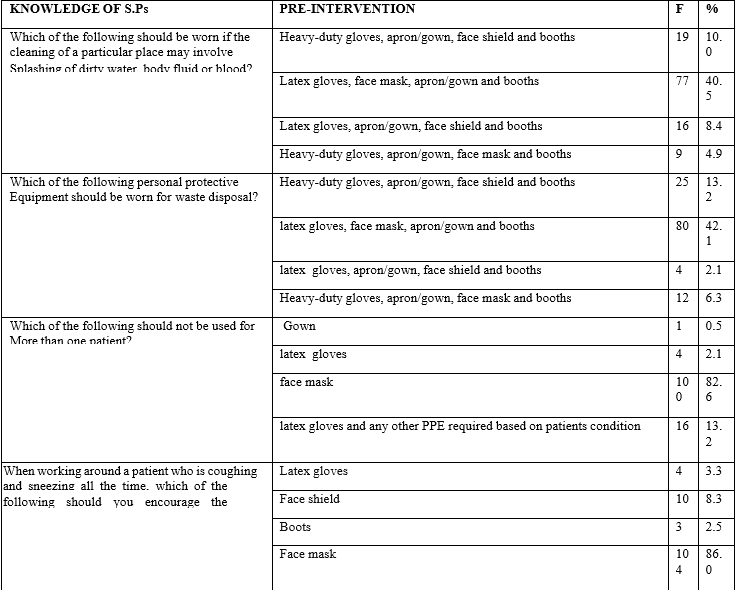
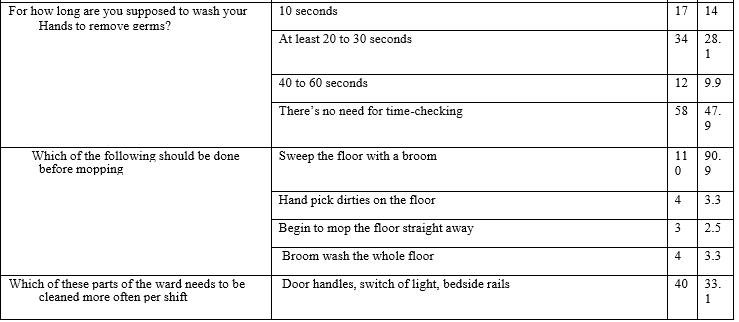
Pre-intervention, only 46 (38.0%) had good knowledge of standard precautions with a mean S.D. (12.033 + 3.47) Table 2a. Far less than one-quarter (10%), knew that heavy-duty gloves, aprons/gowns, face shields, and booths constitute the complete personal protective equipment (PPE) for a terminal cleaning or a cleaning that might involve the splashing of dirty water, body fluid or blood. A few 25(13.2%) knew that heavy duty rubber glove is the most appropriate gloves for medical waste disposal, 4(2.1%) knew that latex gloves should not be used for more than one patient, 110(90.9%) sweeps the ward with a broom, 40 (33.1%) knows that the door handles, light switches and bedrails are among the area that required frequent cleaning and disinfection per shift,
35(28.9%) knows how blood/body fluid spills should be adequately taken care of 105(86.6%) knows that the safety box is the appropriate container for the collection of sharps, Table 2b.
Pre-intervention, 29 (23.9%) self-reported good practices of standard precautions with a mean + SD (13.041 + 2.71) Table 2a. None of the ancillary healthcare workers 121(100%), had a personal heavy duty gloves, a few 13(6.8%) wears face shield when the cleaning of a particular place may involve splashing of dirty water, 25(20.7%) wear heavy duty rubber gloves for waste disposal, majority 107 (88.4%) washes hands after the removal of gloves, a few 27(22.3%) waits for 10 minutes for disinfectant to take effect on a blood/ body fluid stained surface, only a few 23(19%) perform a routine cleaning of highly torched surfaces such as the door knobs, bed rails and light switches of the ward and a Majority 117 ( 96.7%) uses a single bucket system for mopping, Table 3b. Fewer participants, 20(16.5%), displayed good practices on observation with a mean + SD of 7.355+ 1.51 Table 4a.
Post-intervention, a greater number 103(85.1%) of participants acquired good knowledge of standard precautions. There was a significant difference between the pre- and post-intervention knowledge mean scores of standard precautions among the ancillary healthcare workers, Table 2a. There was a significant difference between the pre- and post-intervention self-reported practice mean score, (t = 13.995, P = 0.0001), Table 3a. The overall mean score of observed practices of standard precautions improved from 7.355+ 1.51 to 13.231+4.54 post- intervention with a mean difference of 5.88 and a higher number of participants, 80(66.1%), displaying good practices of standard precautions. There was a significant difference between the pre- and post-intervention observed practice mean score of standard precautions among the ancillary healthcare workers (t = 13.509, P = 0.0001), Table 4a.
Table 1a: Socio-Demographic Characteristics of the Respondent
1b Training on standard precautions
Table 1b: Training on standard precautions among AHCWs
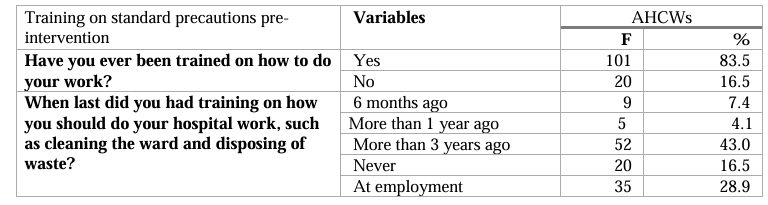
Table 2a showing the pre and post-intervention knowledge of participants
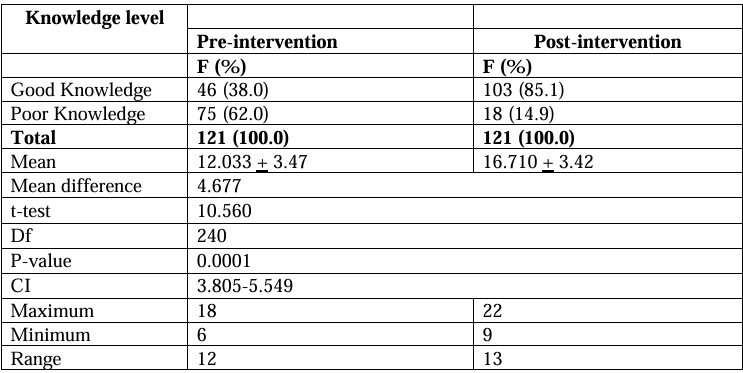
Scores: Poor knowledge (1-11); Good Knowledge (12-22)
Table 2a shows that the pre-intervention knowledge mean score of the participants was 12.033 + 3.47, which became 16.71 + 3.42 post-intervention with a mean difference of
Table 2b Pre-Intervention Knowledge of Standard Precautions among the Ancillary Healthcare Workers
Multiple choice questions
Table 3a showing the Pre and post-intervention self-reported practices of standard precautions among participants
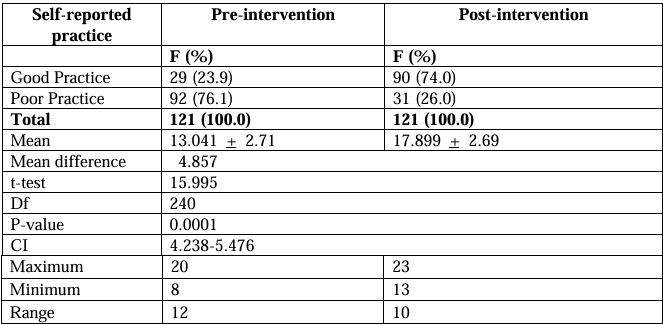
Table 3b Pre-intervention self-reported practices of standard precautions
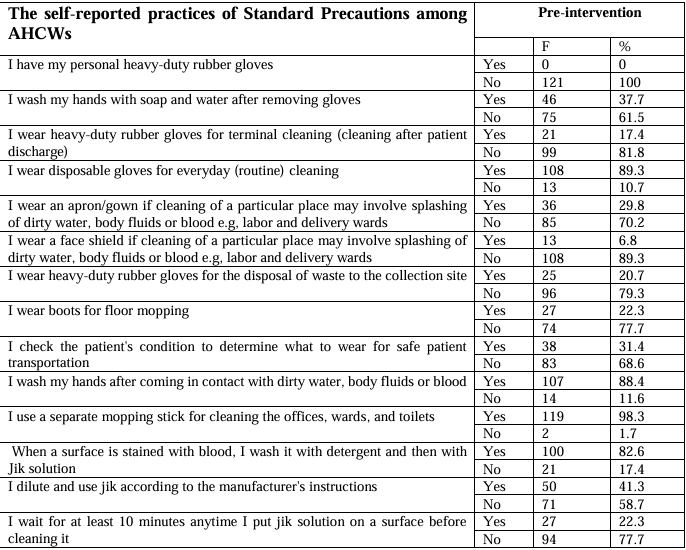
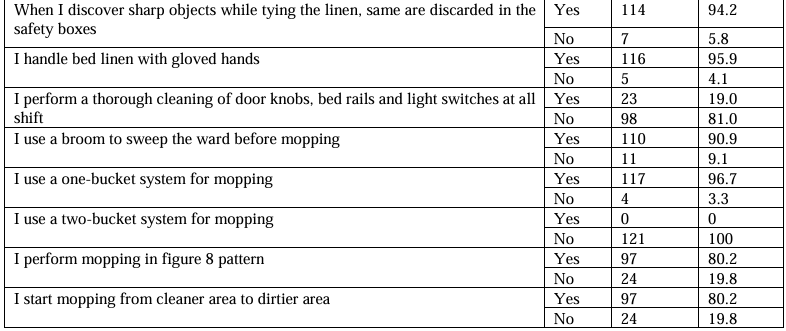
Table 4a Pre and post-intervention observed practices of standard precautions among participants
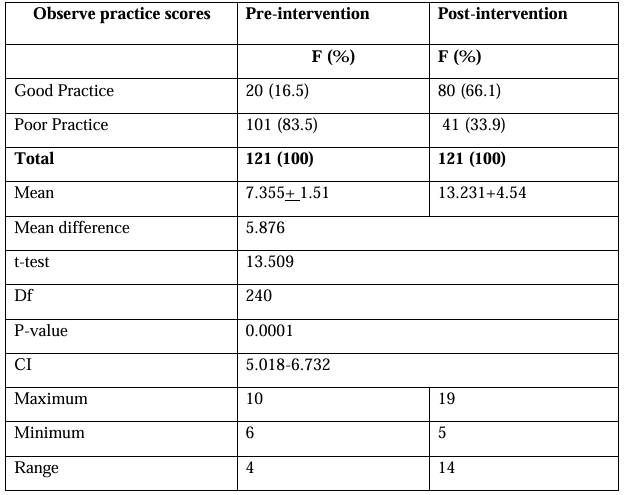
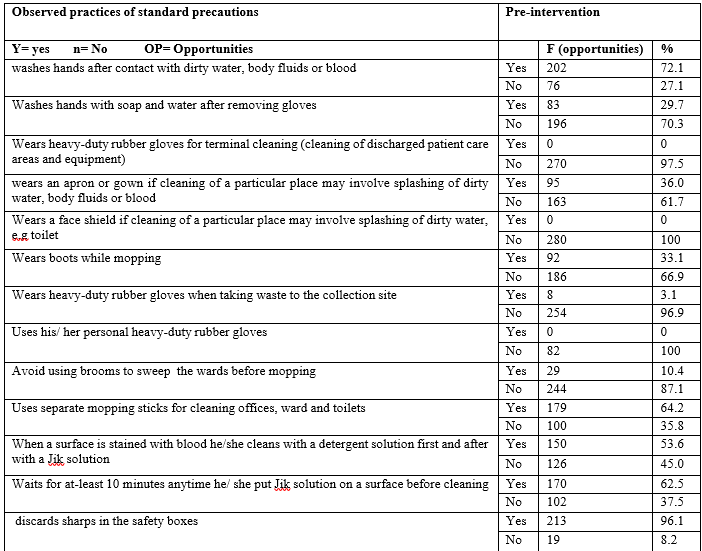
Table 4b Pre-intervention observed practices of standard precautions among participants
Discussion
The study findings revealed that more than 50% of the participants are older adults, predominantly females and married individuals, indicating that while all healthcare workers are at higher risk of HAIs, this particular population faces an even higher risk due to age-related declines in immunity. Consequently, adherence to standard precautions is crucial to safeguarding both the workers and the communities they return to after their daily routines. Also, despite their older age, nearly half of the participants had attained tertiary education, equipping them with the ability to quickly grasp new concepts and effectively transfer knowledge to others. However, the majority had not received training on standard precautions in over three years, indicating a gap in their preparedness for infection control. Therefore, the implemented nurse-led training package will not only enhance their competency in applying standard precautions but also strengthen their capacity to train both current and future staff, reinforcing its overall value.
In support of the findings from this study, Ndu et al. [24] reported, in their study on hand hygiene knowledge and practices among healthcare workers, including ancillary healthcare workers, an age range of 19 to 59 years. The work of Tesfaye et al [41] in his study on infection prevention, control practices and associated factors among healthcare cleaners also supported that the majority of the AHCWs were females and married. In contrast to the findings of this study, Abalkhali et al [42] reported a younger age range of 22-34 years for AHCWs, who are predominantly male, with more than 6 years of experience, in their quasi- experimental study on waste management among AHCWs. This disparity might be as a result of societal expectations regarding physically demanding roles like waste management.
This study revealed that, at the pre- intervention stage, a bit above one-quarter of participants had a good level of knowledge regarding standard precautions. This may be attributed to the older age group that dominated the study population. Although they were more educated, they may not have been as actively engaged or proficient in using digital devices, which provide access to educational resources on social media and various online platforms apart from traditional physical training. The baseline percentages of ancillary healthcare workers with good knowledge of standard precautions in this study were higher than the findings of Osagiede et al. [43], who reported that none of the AHCWs in public primary and secondary health facilities had good knowledge of standard precautions. This difference could be attributed to the disparity in research settings. This study was conducted in a teaching hospital, a tertiary- level facility where continuous education and exposure to updated medical practices are more prevalent in contrast to primary and secondary healthcare facility levels where Osagiede et al [43] conducted their study. This might have contributed to better baseline knowledge of standard precautions among the participants.
Following the intervention, the participants demonstrated a significant improvement in their mean knowledge scores. These findings indicated that the educational intervention was effective in improving the knowledge levels of the participants. This finding is supported by the finding of Battan et al [44], who revealed a significant improvement in the post-intervention performance of staff after training sections focusing on standard precautions specific to the roles of the ancillary healthcare workers.
The study findings revealed that a lower proportion of the participants reported good practice of standard precautions at the pre- intervention stage. None of the participants had personal heavy-duty rubber gloves, few wear heavy-duty rubber gloves for terminal cleaning and waste disposal, the majority did not know how to manage blood or body fluid stains and use disinfectant appropriately. These findings is in tandem with the pre- intervention findings of Singh et al [45] and Kandeel et al [46] where almost all of the AHCWs do not wear necessary PPE for cleaning. These practices are in contrast with the specification of the CDC [38], which stated that heavy-duty rubber gloves should be used in the above scenarios and disinfectant constituted according to the manufacturer’s guide. This might be due to organizational issues of poor provision of PPE and poor understanding of its importance in infection prevention among the AHCWs as a result of their poor training. Also, less than 50% of the participants perform hand hygiene after removal of any type of gloves, though the majority claimed that they do when their hands are exposed to body fluids. This finding is in tandem with the findings of He et al [27] where hand hygiene compliance among the hospital cleaning staff was below 50% pre- intervention but in contrast with the findings of Kielar et al [47] where hand hygiene pre- intervention among the AHCWs was as low as 9%. This might be due to higher educational qualification of this study population.
This study also revealed that a single bucket system is still being used for mopping and the majority of the AHCWs do not routinely clean the highly torched surface areas. This is in tandem with the findings of Singh et al [45] where almost all the AHCWs had poor cleaning practices of highly torched areas pre-intervention.
After the study intervention, the participants showed increased self-reported practices. The mean standard precaution self-reported practice scores of the participants showed a marked increase. These results suggest that the educational intervention significantly enhanced the self-reported practices of standard precautions of the participants. In tandem with this, studies of Mitchell et al. [46] Singh et al[45], and Battan et al. [44] showed improvement in the practice of standard precautions in those specified areas following educational intervention programs among the ancillary healthcare workers. This showed that the knowledge of the participants reinforced by educational intervention has significantly improved compliance with standard precautions. Findings for the observed practices further showed that less than a quarter of the participant had good practices of standard precautions, as a lower percentage of them had good observed practices of standard precautions compared to their self-reported practices pre-intervention. This was in agreement but higher than the findings of Kielar et al. [47], who reported that almost all the ancillary healthcare workers had poor observed practices of standard precautions pre-intervention. This might be attributed to a higher educational qualification of this research population. However, after the intervention, the percentage of participants with good observed practices in the various aspects of S.Ps increased significantly. The observed practice mean scores further support these findings. These results indicate that the participants exhibited more significant changes in observed practices.
Conclusion
The Nurse-led intervention demonstrated a positive impact, particularly in enhancing knowledge, narrowing the gaps in the pre and post intervention self-reported and observed practices of standard precautions.
Limitation
This study was conducted in a single teaching hospital which may limit the generalizability of the findings to other healthcare settings.
Recommendations
Standard precaution intervention package including the provision of its roles specific commodities and equipment should be sustained routinely and expanded to other ancillary healthcare workers and other levels of healthcare settings to replicate its success.
REFERENCES
Centers for Disease Control and Prevention. Cleaning and disinfecting your facility. Centers for Disease Control and Prevention. 2022. Available from: https://www.cdc.gov/hygiene/cleaning/facility.html
Silva RP, Valente GSC, Camacho ACLF. Risk management in the scope of nursing professionals in the hospital setting. Revista Brasileira de Enfermagem. 2020; 73(6).
Brennan D. Common Causes of Nosocomial Infection. Clinical Microbiology: Open Access. 2022
Jun 1; 11(5):1–1. Available from: https://www.walshmedicalmedia.com/open- access/common-causes-of-nosocomial-infection-112027.html
Enaigbe AA, Irodi CC. A review on healthcare-acquired infections of the hospital staff during routine patient’s delivery service. Journal of Applied Sciences and Environmental Management. 2021 Dec 28; 25 (9):1581–6.
Balasubramanian R, Van Boeckel TP, Carmeli Y, Cosgrove S, Laxminarayan R. Global incidence in hospital-associated infections resistant to antibiotics: An analysis of point prevalence surveys from 99 countries. PLoS medicine. 2023 20(6):e1004178. Available from: https://pubmed.ncbi.nlm.nih.gov/37310933/
World Health Organization. WHO launches first ever global report on infection prevention and control [Internet]. World Health Organisation. 2022. Available from: https://www.who.int/news/item/06-05-2022-who-launches-first-ever-global-report-on- infection-prevention-and-control
Abubakar U, Amir O, Rodríguez-Baño J. Healthcare-associated infections in Africa: a systematic review and meta-analysis of point prevalence studies. Journal of Pharmaceutical Policy and Practice. 2022 Dec 9; 15(1).
Abubakar U. Point-prevalence survey of hospital-acquired infections in three acute care hospitals in Northern Nigeria. Antimicrobial Resistance & Infection Control. 2020 May 11; 9(1).
Ige O, Asuzu M, Adesanmi A. Hospital-acquired infections in a Nigerian tertiary health facility: An audit of surveillance reports. Nigerian Medical Journal. 2011; 52(4):239. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3329093/
Aryal S. Mode of Transmission of Diseases- Direct and Indirect Transmission [Internet]. The Biology Notes. 2021. Available from: https://thebiologynotes.com/mode-of-transmission-of-diseases/
Sikora A, Zahra F. Nosocomial Infections [Internet]. PubMed. Treasure Island (FL): StatPearls Publishing; 2023. Available from: https://www.ncbi.nlm.nih.gov/books/NBK559312/
Centers for Disease Control and Prevention. Appendix D: Linen and Laundry Management | Environmental Cleaning in RLS | HAI | CDC [Internet]. www.cdc.gov. 2020. Available from: https://www.cdc.gov/hai/prevent/resource-limited/laundry.html
Janik-Karpinska E, Brancaleoni R, Niemcewicz M, Wojtas W, Foco M, Podogrocki M, et al.
Healthcare Waste—A Serious Problem for Global Health. Healthcare. 2023 Jan 13; 11(2):242.
Kobos L, Anderson K, Kurth L, Liang X, Groth CP, England L, et al. Characterization of Cleaning and Disinfection Product Use, Glove Use, and Skin Disorders by Healthcare Occupations in a Midwestern Healthcare Facility. Buildings. 2022 Dec 14; 12(12):2216.
Walton A, Rogers B. Workplace Hazards Faced by Nursing Assistants in the United States: A Focused Literature Review. International Journal of Environmental Research and Public Health. 2017 May 19; 14(5):544.
United States Bureau of Labor Statistics. Nursing Assistants and Orderlies: Occupational Outlook Handbook: U.S. Bureau of Labor Statistics. Bls.gov. 2019. Available from: https://www.bls.gov/ooh/healthcare/nursing-assistants.htm
Joseph B, Joseph M. The health of the healthcare workers. Indian Journal of Occupational and Environmental Medicine. 2019; 20(2):71–2. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5299814/
Wee LE, Sim JXY, Conceicao EP, Aung MK, Ng IM, Ling ML. Re: “Personal protective equipment protecting healthcare workers in the Chinese epicenter of COVID-19” by Zhao et al.. Clinical Microbiology and Infection. 2020; 26(12):1719–21.
Praisie R, D Anandadurai, Nelson SB, Sriandaal Venkateshvaran, Manoje Thulasiram. Profile of Splash, Sharp and Needle-Stick Injuries among Healthcare Workers in a Tertiary Care Hospital in Southern India. Cureus. 2023 Jul 29; 15(7).
Department of Health Victoria. Infection control – standard and transmission-based precautions.
Infection control – standard and transmission-based precautions. 2023. Available from:
https://www.health.vic.gov.au/infectious-diseases/infection-control-standard-and- transmission-based-precautions
Padmanabhan KK, Barik D. Health hazards of medical waste and its disposal. Energy from Toxic Organic Waste for Heat and Power Generation. 2019; 99–118.
Onyedibe KI, Shehu NY, Pires D, Isa SE, Okolo MO, Gomerep SS, et al. Assessment of hand hygiene facilities and staff compliance in a large tertiary health care facility in northern Nigeria: a cross-sectional study. Antimicrobial Resistance & Infection Control. 2020; 9(1).
Grejo CS, Gambero ML, Marini LA, Bueno ACR, Silva DA da, Roncon CM, et al. Higienização das mãos em unidades de terapia intensiva neonatal, pediátrica e adulto. Revista de Medicina. 2022 Sep 2; 101(5).
Ndu Anne, C., Arinze-Onyia, S. U., & Aguwa, E. N. Hand Hygiene: Knowledge and Practice by Health Care Workers: Nigerian Journal of Medicine. LWW. 2017. Available from: https://journals.lww.com/njom/Abstract/2017/26040/Hand_Hygiene Knowledge_And_ Practice_By_Health.4.aspx.
Banjo, Onajobi H. Hygiene Status of Disinfecting Solutions Used in Floor Cleaning of Five Selected Hospitals in Ogun State, South Western, Nigeria. Nigerian Journal of Microbiology. 2019; 33(1):4357–63. Available from: https://nsmjournal.org.ng/2019-33-1/02.pdf
Huang F, Boudjema S, Brouqui P. Three-Year hand hygiene monitoring and impact of real-time reminders on compliance. Journal of Hospital Infection. 2021; 117.
He W, Chen X, Cheng X, Li Y, Feng B, Wang Y. Exploring the effect of novel six moments on hand hygiene compliance among hospital cleaning staff members: a quasi-experimental study. Epidemiology and Infection. 2023; 151(73).
Ghorbanmovahhed S, Shahbazi S, Gilani N, Ostadi A, Shabanloei R, Gholizadeh L. Effectiveness of implementing an infection control link nurse program to improve compliance with standard precautions and hand hygiene among nurses: a quasi-experimental study. BMC Medical Education. 2023 Apr 19; 23(1).
Farotimi A, Nwozichi C, Ajao E, Ademuyiwa I. Effect of training on knowledge, perception, and risk reduction regarding infection control among nurses in selected teaching hospitals in Nigeria. Iranian Journal of Nursing and Midwifery Research. 2018; 23(6):471.
Ogbondah BO. Effect of Health Education Intervention on Knowledge of Universal Safety Precautions among Primary Health Care Workers in Rivers State, Nigeria. The Nigerian Health Journal. 2020; 20(3):111–21. Available from: https://www.tnhjph.com/index.php/tnhj/article/view/490
Angeloni NLN, Furlan MCR, Barcelos L da S, Ferreira AM, Sousa AFL de, Valim MD, et al.
Multimodal Educational Intervention for Adherence to Standard Precautions in the COVID-19 Pandemic Among Nursing Professionals: A Quasi-Experimental Study. Journal of Nursing and Midwifery Sciences. 2024; 11(1). Available from: https://brieflands.com/articles/jnms-143516
Uchendu OC, Desmenu AP, Owoaje ET. Effect of training on knowledge and attitude to standard precaution among workers exposed to body fluids in a tertiary institution in south-west Nigeria. Annals of Ibadan Postgraduate Medicine. 2020; 18(2):100–5. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8369401/
Suksatan W, Jasim SA, Widjaja G, Jalil AT, Chupradit S, Ansari MJ, et al. Assessment effects and risk of nosocomial infection and needle stick injuries among patients and health care workers. Toxicology Reports. 2022; 9(ISSN 2214-7500):284–92. Available from: https://www.sciencedirect.com/science/article/pii/S2214750022000233
Berhan Z, Malede A, Gizeyatu A, Sisay T, Lingerew M, Kloos H, et al. Prevalence and associated factors of needle stick and sharps injuries among healthcare workers in northwestern Ethiopia. Gurgel RQ, editor. PLOS ONE. 2021; 16(9):e0252039. Available from: https://journals.plos.org/plosone/article?id=10.1371%2Fjournal.pone.0252039
Leistner R, Kohlmorgen B, Brodzinski A, Schwab F, Lemke E, Gregor Zakonsky, et al.
Environmental cleaning to prevent hospital-acquired infections on non-intensive care units: a pragmatic, single-center, cluster randomized controlled, crossover trial comparing soap-based disinfection and probiotic cleaning. eClinicalMedicine. 2023; 59: 101958–8.
Mahamat G, Kenmoe S, Akazong EW, Ebogo-Belobo JT, Mbaga DS, Bowo-Ngandji A, et al.
Global prevalence of hepatitis B virus serological markers among healthcare workers: Asystematic review and meta-analysis. World Journal of Hepatology. 2021; 13(9):1190–202.
World Health Organization. Hand Hygiene Technical Reference Manual after body [Internet].
Centers for Disease Control and Prevention. Environmental Cleaning Procedures. Healthcare- Associated Infections (HAIs). 2024. Available from: https://www.cdc.gov/healthcare- associated-infections/hcp/cleaning-global/procedures.html
Centers for Disease Control and Prevention. CDC’s Core Infection Prevention and Control Practices for Safe Healthcare Delivery in All Settings. Infection Control. 2024. Available from: https://www.cdc.gov/infection-control/hcp/core-practices/index.html
Occupational Safety and Health Administration. Personal Protective Equipment – Overview | Occupational Safety and Health Administration. Osha.gov. 2023. Available from: https://www.osha.gov/personal-protective- equipment#:~:text=Personal%20protective%20equipment%20is%20addressed
Tesfaye AH, Mekonnen TH, Desye B, Yenealem DG. Infection Prevention and Control Practices and Associated Factors among Healthcare Cleaners in Gondar City: An Analysis of a Cross-Sectional Survey in Ethiopia. Risk Management and Healthcare Policy; 16: 1317– Available from: https://www.dovepress.com/infection-prevention-and-control-practices-and- associated-factors-amon-peer-reviewed-fulltext-article-RMHP
Abalkhail A, Kabir R, Elmosaad Y, Alwashmi A, Alhumaydhi F, Alslamah T, et al. Citation. Int
J Environ Res Public Health. 2022; 19(10). Available from: https://www.mdpi.com/1660-4601/19/10/6342/pdf?version=1653376362
Osagiede E, Utomi S, Egbuta O, Osagiede E, Airefetalor I, Abah S. Knowledge and Practice of Standard Precautions for Infection Prevention and Control among Health Care Workers in Public Primary and Secondary Health Facilities in Edo State: A Reflection of the Neglect of First and Second Levels of Care in Infection Preve. Journal of BioMedical Research and Clinical Practice. 2020 Dec 24; 3(4):435–43.
Battan RM, Kattan WM, Saqr RR, Alawi M. The effectiveness of simulation-based training on KAU hospital housekeeping staff performance. Infection, Disease & Health [Internet].
2023 Mar 3; 28(3). Available from: https://reader.elsevier.com/reader/sd/pii/S2468045123000123?token=6B4BCF73C3F7D12C520130C99C6A076AACB7A4A3E51DFC7288FB1117F44469A28E7346DFF063684207454B9276873614&originRegion=eu-west-1&originCreation=20230311235706
Singh V, Narula H, Supehia S, Sharma M, Gupta PK, Sharma A, et al. Impact of Video Modules Based Training on Knowledge, Attitude, and Practices of Cleaning and Disinfection Among Housekeeping Staff at a Tertiary Care Center During the COVID-19 Pandemic. Cureus. 2021; 13(10). Available from: https://www.cureus.com/articles/73926-impact-of- video-modules-based-training-on-knowledge-attitude-and-practices-of-cleaning-and- disinfection-among-housekeeping-staff-at-a-tertiary-care-center-during-the-covid-19- pandemic
Kandeel A, Abdel-Hady El-Gilany. Needle stick and sharp injuries (NSSIs) among housekeepers in a Saudi hospital: An intervention study. International Journal of Infection Control [Internet]. 2017 Jul 20; 13(1):i1. Available from: https://www.researchgate.net/publication/318598746_Needle_stick_and_sharp_injuries_ NSSIs_among_housekeepers_in_a_Saudi_hospital_An_intervention_study
Mitchell BG, Hall L, White N, Barnett AG, Halton K, Paterson DL, et al. An environmental cleaning bundle and health-care-associated infections in hospitals (REACH): a multicentre, randomised trial. The Lancet Infectious Diseases. 2019 (4):410–8.
Kielar M, Depurbaix R, Agnyziak M, Wijaszka B, Poboży T. The COVID-19 pandemic as a factor of hospital staff compliance with the rules of hand hygiene: assessment of the usefulness of the “Clean Care is a Safer Care” program as a tool to enhance compliance with hand hygiene principles in hospitals. Journal of Preventive Medicine and Hygiene. 2021;62(1):E25–32. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8283626/
© 2025 Integrated Journal of Medicine and Medical Sciences. All rights reserved.